The liver is the body’s primary filtration system, responsible for metabolizing drugs, detoxifying blood, and synthesizing vital proteins. In the context of performance-enhancing drugs (PEDs), the liver is often the first organ to suffer significant damage.
When discussing Anabolic-Androgenic Steroids (AAS), the question “Which steroid is hardest on the liver?” is common. While individual responses vary based on genetics and existing health, certain compounds are chemically engineered in a way that makes them inherently more hepatotoxic than others.
To understand why some steroids destroy liver cells (hepatocytes) while others (like injectable testosterone) have minimal impact, we must first look at the chemistry of survival.

Natural testosterone is quickly destroyed by the liver. If you were to swallow a pill of pure testosterone, the liver would break it down before it ever reached the bloodstream to exert an effect. This is known as the “first-pass metabolism.”
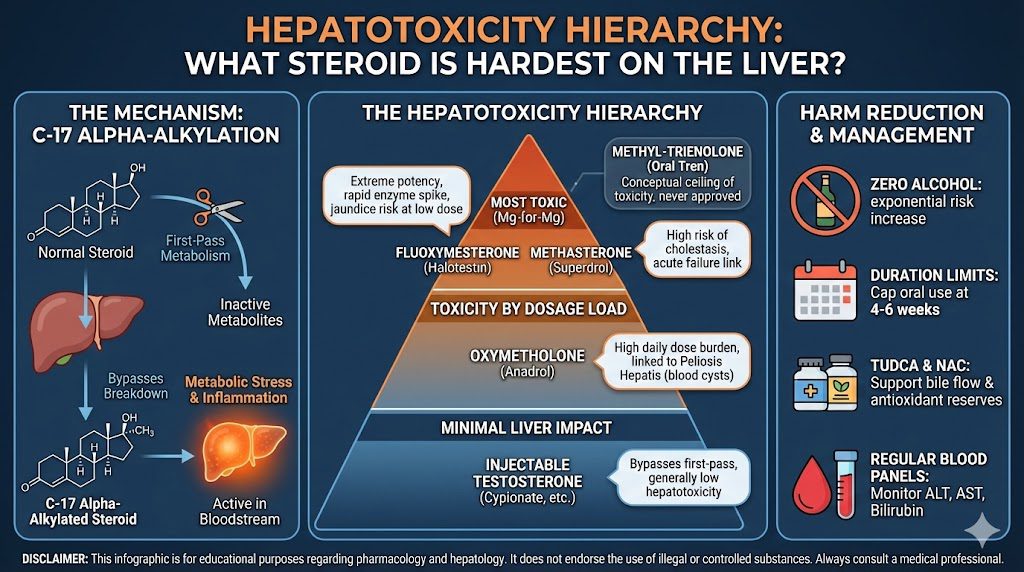
To bypass this defense mechanism, pharmaceutical chemists in the mid-20th century developed a process called C-17 Alpha-Alkylation (C17-aa). By adding an alkyl group (a methyl or ethyl group) to the 17th carbon position of the steroid molecule, the drug becomes resistant to hepatic breakdown.
This modification allows the steroid to survive the first pass through the liver and enter the bloodstream active. However, this survival comes at a steep price: the inability of the liver to break the substance down places immense metabolic stress on the organ. The steroid effectively acts as a cumulative toxin, causing inflammation, enzyme elevation, and potential cell death.
Almost all oral steroids (Dianabol, Anadrol, Winstrol) are C17-aa. However, among this group, a hierarchy of toxicity exists.
While “toxicity” can be measured in different ways (mg per mg potency vs. total dosage load), three compounds consistently rank as the most destructive to hepatic health in medical literature and anecdotal case studies.
If one were to identify the single harshest pharmaceutical-grade steroid on the liver, Halotestin is the frequent answer.
Technically a “designer steroid,” Superdrol (Methyldrostanolone) was sold legally as a prohormone in the mid-2000s before being banned. Despite its legal past, it is widely regarded as one of the most hepatotoxic compounds ever sold.
Anadrol is often cited as the “king” of mass builders, but its reputation for liver damage is complex.
Though rarely seen and never medically approved for human use, Methyl-Trienolone deserves mention as perhaps the most toxic steroid conceptually. It is an oral version of Trenbolone. In clinical trials (for research), it was found to be so hepatotoxic that it was never released as a human drug. It is considered the absolute ceiling of liver toxicity, capable of causing jaundice in as little as a week.
It is important to understand that “liver damage” is not a single condition. Steroids cause specific pathologies.
This is the most common and earliest sign. When liver cells are stressed or die, they leak enzymes (Alanine Transaminase [ALT] and Aspartate Transaminase [AST]) into the bloodstream.
Common with Superdrol and Winstrol.
This is a rare but potentially fatal condition strongly associated with Anadrol and long-term oral steroid use.
These are benign liver tumors. While not cancerous initially, they can grow large enough to rupture or, in rare cases, transform into Hepatocellular Carcinoma (liver cancer).
A common misconception is that all steroids hurt the liver. This is false.
Injectable bio-identical Testosterone (Cypionate, Enanthate) bypasses the first pass of the liver. It enters the bloodstream directly from the muscle tissue. While massive doses can cause minor stress, therapeutic or moderate doses of injectable testosterone generally have a negligible impact on liver values.
The danger arises almost exclusively when users introduce oral compounds or specific veterinary injectables (like Winstrol Depot) that are chemically structured to act like orals.
For those who choose to use these compounds despite the risks, harm reduction focuses on supporting the liver’s ability to filter toxins.
Combining C17-aa steroids with alcohol is akin to pouring gasoline on a fire. Both compete for the same metabolic pathways. The combination exponentially increases the risk of acute liver failure.
Clinical literature suggests that hepatotoxic agents should rarely be used for longer than 4 to 6 weeks. The popular “12-week oral cycle” is a recipe for severe cholestasis.
You cannot “feel” liver enzymes rising until it is too late (jaundice). The only way to detect stress is through blood work monitoring ALT, AST, GGT, and Bilirubin levels.
When analyzing the hierarchy of hepatotoxicity, Halotestin and Superdrol generally claim the title for the most toxic compounds milligram-for-milligram, capable of causing rapid enzyme spikes and cholestasis. Anadrol follows closely due to the sheer volume of substance the liver must process.
However, the “hardest” steroid on the liver is ultimately the one taken without respect for physiology. Even milder compounds like Anavar (Oxandrolone) can cause damage if taken at high doses for months on end.
The liver is resilient and can regenerate, but it is not invincible. The physiological cost of oral anabolic steroids is a debt that must eventually be paid, often in the form of scarring, cysts, or chronic dysfunction. For this reason, the medical community universally advises against the non-therapeutic use of C17-alpha-alkylated androgens.