
The decision to transition from natural training to utilizing anabolic-androgenic steroids (AAS) is not merely a step up in a fitness routine; it is a fundamental, systemic alteration of the body’s endocrine system. In the world of performance enhancement, the line between calculated biological optimization and reckless physiological damage is incredibly thin.
For those researching how a first steroid cycle is structured, the internet is often a minefield of conflicting “bro-science,” outdated forum advice, and dangerous protocols. This article provides a strictly informational breakdown of the biological mechanics, standard community protocols, and harm-reduction strategies involved in understanding a first steroid cycle.
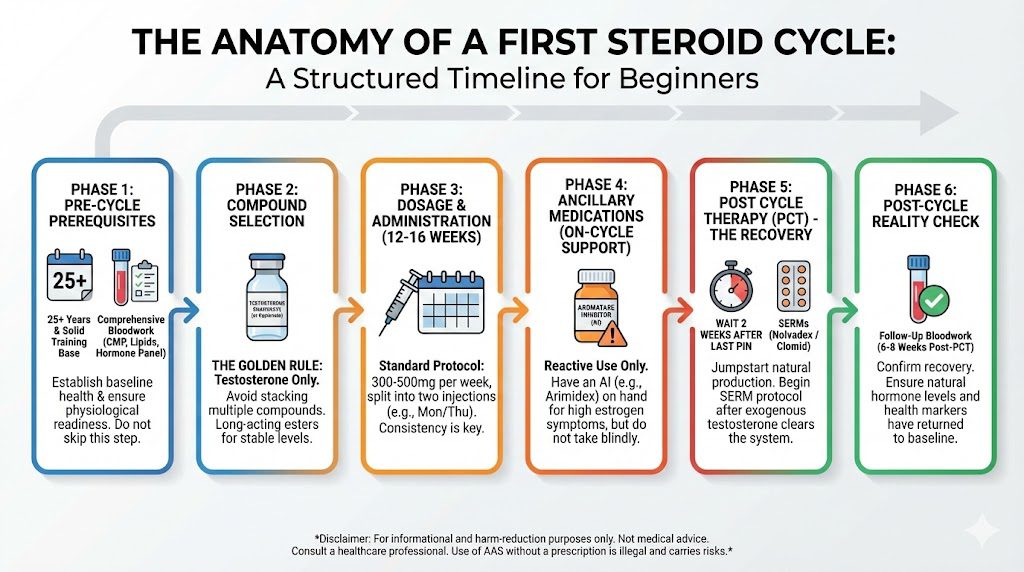
Phase 1: The Pre-Cycle Prerequisites
Before a needle ever pierces the skin, a physiological foundation must be established. The introduction of exogenous hormones stresses the cardiovascular system, the liver, the kidneys, and the hypothalamic-pituitary-gonadal (HPG) axis. Without a proper baseline, an athlete is flying blind into potentially permanent health issues.
1. The Biological and Training Baseline Endocrinologists and harm-reduction experts generally advise against the use of AAS before the mid-twenties. Until roughly age 25, the male brain (specifically the prefrontal cortex) and the endocrine system are still developing. Introducing suppressive compounds too early can cause permanent alterations to natural testosterone production. Furthermore, a user should have several years of consistent, progressive training and a dialed-in nutritional protocol. Steroids amplify existing habits; they do not fix broken ones.
2. Comprehensive Bloodwork (The Internal Audit) Bloodwork is the only objective measure of internal health. A “before” snapshot is mandatory so the user knows what their baseline normal looks like, allowing them to return to it post-cycle. Essential pre-cycle markers include:
- Comprehensive Metabolic Panel (CMP): To evaluate kidney and liver function (AST, ALT, BUN, Creatinine).
- Lipid Panel: Steroids notoriously crush HDL (good cholesterol) and elevate LDL (bad cholesterol). A baseline is critical.
- Complete Blood Count (CBC): To monitor hematocrit and red blood cell count, as AAS stimulate red blood cell production, potentially thickening the blood.
- Hormone Panel: Total Testosterone, Free Testosterone, Estradiol (E2), Luteinizing Hormone (LH), Follicle-Stimulating Hormone (FSH), and Prolactin.
Phase 2: Compound Selection – The “Testosterone Only” Philosophy
When looking at the vast array of available compounds—Trenbolone, Dianabol, Deca Durabolin, Winstrol—the temptation for a beginner is to stack multiple drugs to maximise gains. Biologically, this is the worst possible approach.
The Golden Rule: One Compound at a Time The human body reacts uniquely to different exogenous hormones. If a user stacks Testosterone, Deca, and Dianabol on their first cycle and develops severe acne, erectile dysfunction, or panic-inducing blood pressure spikes, it is impossible to pinpoint which compound is causing the side effect.
For this reason, the universal standard for a first cycle in the performance community is Testosterone only. Testosterone is the hormone the male body already produces and recognizes. It is highly effective for building muscle, highly tolerable, and provides a clear baseline for how the user’s body reacts to supraphysiological (above natural) hormone levels.
Understanding Esters Testosterone is attached to an ester, which dictates how slowly the hormone is released into the bloodstream.
- Testosterone Enanthate and Cypionate: These are long-acting esters. They require less frequent injections (typically twice a week) and maintain highly stable blood serum levels. They are the standard recommendation for a first cycle.
- Testosterone Propionate: A short-acting ester requiring every-other-day (EOD) injections. While it clears the system faster (which is helpful if side effects occur), the injection frequency is usually too burdensome and causes too much blood level fluctuation for a beginner.
Phase 3: Dosage, Duration, and Administration
The mechanics of the cycle involve balancing the dose to maximise protein synthesis while minimizing androgenic and estrogenic side effects.
1. The Dosage In a clinical setting (TRT – Testosterone Replacement Therapy), doctors prescribe 100mg to 200mg per week to put a man into the normal physiological range. In the performance enhancement community, a standard first cycle pushes the body into a supraphysiological state. Typically, this ranges from 300mg to 500mg per week.
- 300mg/week: Often referred to as a “sports TRT” or highly conservative cycle. It yields significant gains over a natural baseline with a very low risk of severe side effects.
- 500mg/week: The traditional bodybuilding standard for a first cycle. It provides maximum initial muscle tissue accrual but dramatically increases the likelihood of needing ancillary medications to manage side effects.
2. The Duration A standard first cycle lasts between 12 to 16 weeks. Why not shorter? Long-acting esters like Enanthate take 4 to 5 weeks to reach peak blood serum concentration. Stopping at week 8 means the user is aborting the cycle just as the physiological benefits are fully materializing. Why not longer? Beyond 16 weeks, health markers (lipids, hematocrit) begin to degrade significantly, and myostatin (a protein that inhibits muscle growth) rises, diminishing returns.
3. Administration Frequency To avoid severe peaks and valleys in hormone levels—which trigger acne, mood swings, and estrogen spikes—the weekly dosage is split. A 500mg/week protocol is almost always divided into two 250mg injections, typically administered on a Monday/Thursday or Tuesday/Friday schedule.
Phase 4: Ancillary Medications (Managing the Conversion)
Injecting high amounts of testosterone means the body will attempt to maintain homeostasis. It does this through a process called aromatization, where the aromatase enzyme converts excess testosterone into estrogen (Estradiol/E2).
While some estrogen is vital for muscle growth, libido, and joint health, too much leads to high blood pressure, severe water retention, and gynecomastia (the development of breast tissue in men).
Aromatase Inhibitors (AIs) Users mitigate this by keeping an Aromatase Inhibitor on hand. The two most common are:
- Arimidex (Anastrozole): A non-suicidal AI that temporarily binds to the aromatase enzyme.
- Aromasin (Exemestane): A suicidal AI that permanently binds to and disables the enzyme.
The Harm Reduction Protocol: The modern consensus is not to take an AI blindly. Crashing estrogen to zero causes severe joint pain, depression, and lipid destruction. AIs are used reactively—only deployed if bloodwork shows massive estrogen spikes or if the user exhibits physical symptoms like itchy, sensitive nipples.
Phase 5: Post Cycle Therapy (PCT) – The Recovery
When exogenous testosterone enters the body, the brain senses the massive surplus and completely shuts down its natural production. The testicles atrophy (shrink), and luteinizing hormone (LH) drops to zero.
When the 16-week cycle ends, the exogenous testosterone eventually clears the bloodstream. The user is left with no synthetic testosterone and a shut-down natural system. This is the “crash”—characterized by depression, muscle loss, and zero libido.
Post Cycle Therapy (PCT) is the pharmacological intervention used to forcefully restart the body’s natural testosterone production.
1. The Waiting Period A user cannot start PCT the day after their last injection. Testosterone Enanthate takes roughly 14 to 18 days to clear the system. Starting PCT while synthetic testosterone is still suppressing the brain is entirely useless.
2. The PCT Compounds (SERMs) Selective Estrogen Receptor Modulators (SERMs) trick the pituitary gland into producing LH and FSH, signaling the testes to turn back on.
- Nolvadex (Tamoxifen): The gold standard for PCT. A standard protocol might be 40mg per day for two weeks, followed by 20mg per day for two weeks.
- Clomid (Clomiphene): Often used in conjunction with Nolvadex for a highly suppressive cycle, though it carries a higher risk of emotional side effects and visual disturbances.
3. HCG (Human Chorionic Gonadotropin) Advanced users run HCG during the cycle (e.g., 250 IU twice a week). HCG mimics LH, keeping the testicles plump and functioning while the brain is shut down. This makes the eventual PCT phase significantly easier and faster, as the testes do not need to be “woken up” from total atrophy.
Phase 6: The Post-Cycle Reality Check
A cycle is not over when the PCT pills run out. It is over when bloodwork confirms that natural homeostasis has been restored.
Approximately 6 to 8 weeks after the final day of PCT, the user must undergo a complete blood panel identical to the pre-cycle baseline.
- Did natural testosterone levels return to baseline?
- Did the lipid profile recover?
- Are liver and kidney enzymes back in the safe range?
If the numbers have not recovered, the user remains in a state of hypogonadism and may require further medical intervention from an endocrinologist.
Conclusion
Starting a steroid cycle is a profound biochemical commitment. It requires meticulous planning, a willingness to spend heavily on comprehensive bloodwork and ancillary medications, and the discipline to adhere to strict pharmacological protocols.
The most successful researchers and athletes view performance enhancement not as a quick fix, but as a rigid science. Understanding the mechanisms of testosterone, the risks of estrogen conversion, and the vital importance of Post Cycle Therapy is what separates calculated physiological optimization from long-term endocrinological damage.