Steroids give you an edge on strength, muscle density, and recovery. Many people rush in […]…
Navigating AAS Use: Safety, Strategy, and Long-Term Health In the pursuit of the ultimate physique, […]…
When looking to enhance your performance and achieve your fitness goals, buying Canadian anabolics online […]…
Buy HGH Online in Canada: The Ultimate Guide to Sourcing Premium Somatropin When it comes […]…
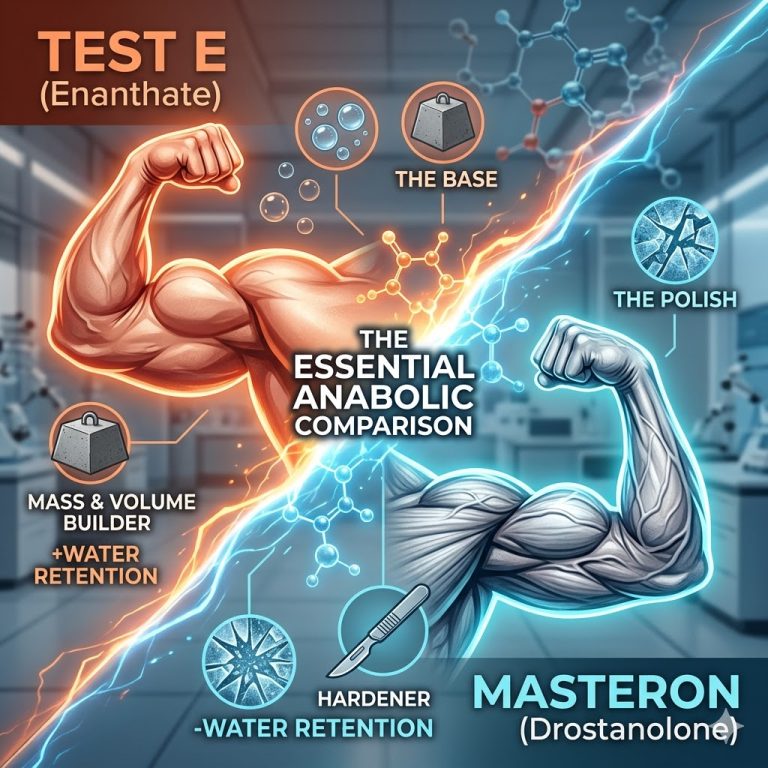
Testosterone Enanthate vs. Masteron Explained In the advanced study of sports pharmacology, compounds are rarely […]…
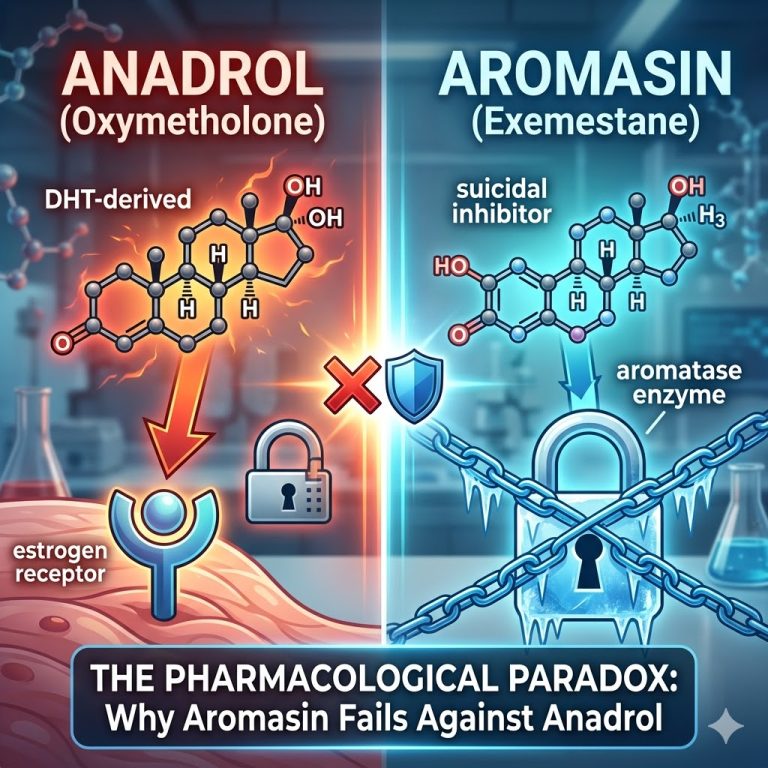
The Pharmacological Paradox: Anadrol vs. Aromasin Explained In the advanced study of sports pharmacology and […]…
How to use the Wolverine Peptide Stack: A Comprehensive Guide to Healing and Regeneration Performance […]…
In the spheres of high-performance athletics, advanced bodybuilding, and regenerative medicine, the ultimate bottleneck has […]…
Struggling with confidence in the bedroom? You’re not alone. Erectile dysfunction (ED) affects millions of […]…