What Anabolics are used for Muscle Gain
For decades, Anabolic-Androgenic Steroids (AAS) have been a subject of intense curiosity and debate. While frequently discussed in gym locker rooms, the actual science behind what these compounds are and how they influence muscle hypertrophy is often obscured by bro-science and misinformation.
To truly understand anabolics, one must move past the slang and look at the pharmacology. This guide breaks down the primary compounds historically used for muscle gain, explaining their mechanisms of action and the physiological reality of their use.
The Foundation: Testosterone
In both medical and performance contexts, Testosterone is the baseline. It is the primary male sex hormone, and all other anabolic steroids are essentially synthetic derivatives of it.
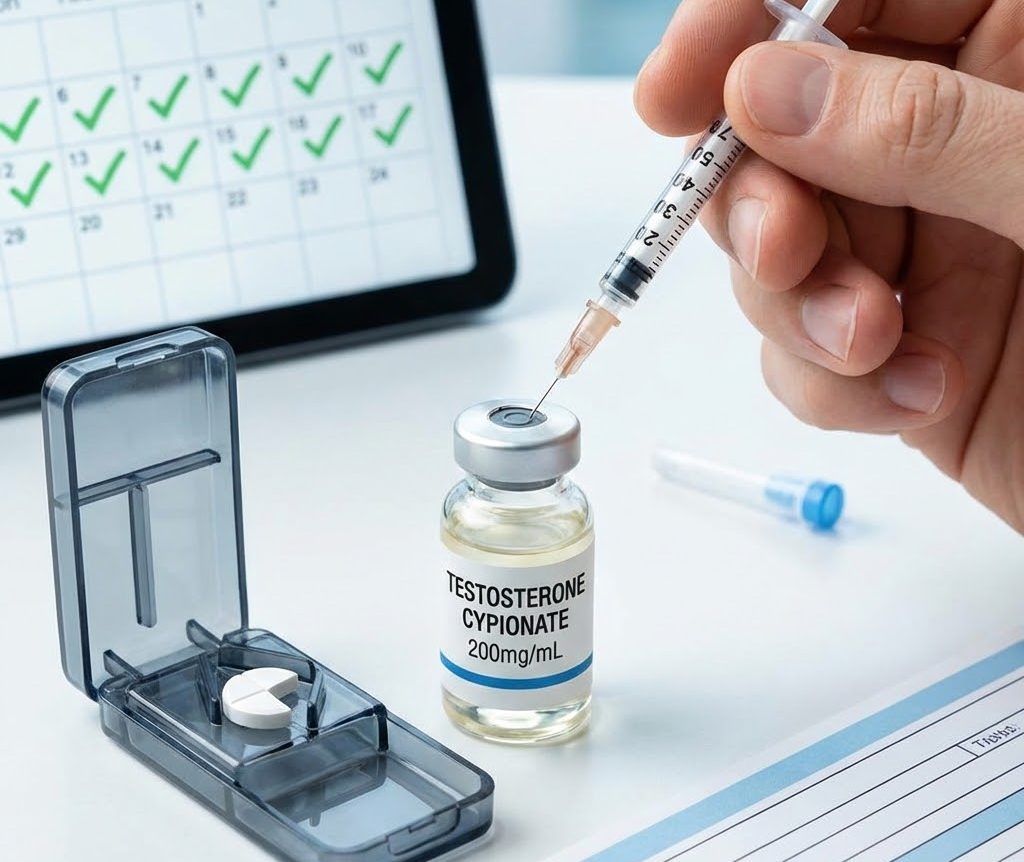
When used for muscle gain, testosterone is typically administered via injection in esterified forms (such as Enanthate, Cypionate, or Propionate). These esters determine how quickly the hormone is released into the bloodstream.
- How it works: Testosterone binds to androgen receptors in muscle tissue, signaling the body to increase protein synthesis and nitrogen retention. Nitrogen is a key component of amino acids (the building blocks of protein); a positive nitrogen balance creates an environment conducive to muscle growth.
- The Role in “Cycles”: In almost all performance-enhancing protocols, testosterone is used as the “base” to replace the natural production that inevitably shuts down when exogenous hormones are introduced.

The administration of anabolic compounds involves strict protocols, though self-injection carries significant risks of infection and tissue damage.
The “Mass Builders”: 19-Nortestosterone Derivatives
This class of steroids is derived by altering the testosterone molecule at the 19th carbon position. These compounds are famously known for their potent anabolic (muscle-building) properties relative to their androgenic (masculinizing) effects.
1. Nandrolone (Deca-Durabolin)
Nandrolone is one of the most widely used anabolics in history.
- Primary Use: It is favored for off-season “bulking” phases. Beyond muscle hypertrophy, it is clinically noted for increasing bone mineral density and collagen synthesis, which some users report provides relief to achy joints during heavy training.
- The Trade-off: Nandrolone is known for its long detection time and significant suppression of the HPTA (Hypothalamic-Pituitary-Testicular Axis), leading to difficult recovery of natural hormones post-use.
2. Trenbolone
Originally developed for veterinary use (to increase feed efficiency in cattle), Trenbolone is considered one of the most powerful anabolics in existence.
- Primary Use: Unlike Nandrolone, Trenbolone does not convert to estrogen (aromatize), meaning it produces very dry, hard muscle gains without water retention.
- Safety Context: The potency comes with a cost. Trenbolone is frequently associated with severe side effects, including cardiovascular strain, sleep disturbances, and acute anxiety. It represents the extreme end of the risk-reward spectrum.
The DHT Derivatives: Hardening and Strength
Derived from Dihydrotestosterone (DHT), these compounds are often used when “dry” gains and strength are prioritized over raw mass.
1. Drostanolone (Masteron)
- Primary Use: historically used in breast cancer treatment, Masteron is now associated with “cutting” phases. It has mild anti-estrogenic properties and is used to provide a “hard” look to the physique. It is generally not used for adding significant mass but for preserving it while dieting.
2. Primobolan (Methenolone)
- Primary Use: Known as a “gentle” steroid, Primobolan is often favored for its safety profile relative to other compounds. It promotes slow, steady nitrogen retention without heavy water weight. It is often cited in the context of “lean bulk” cycles where quality of tissue is preferred over quantity.
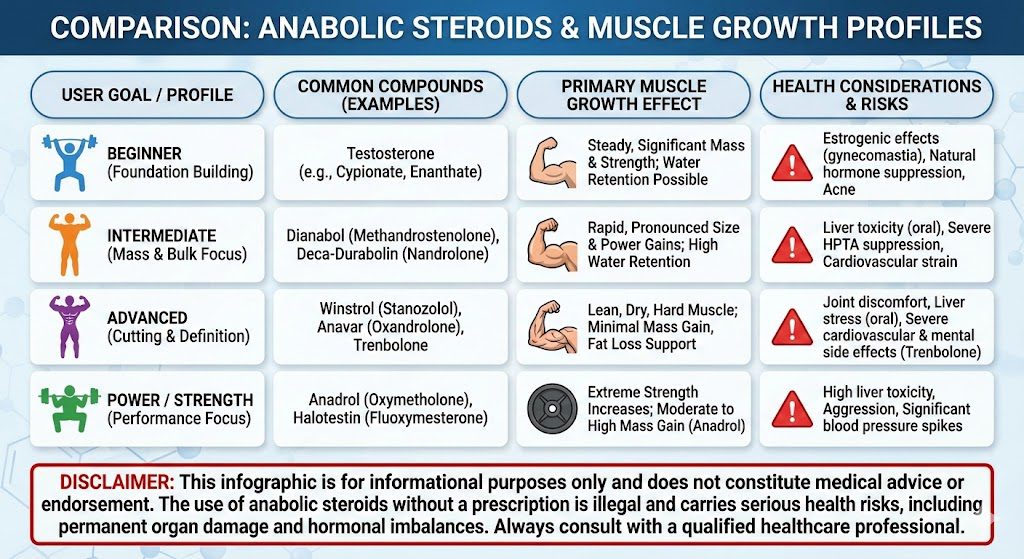
A visual breakdown of common anabolic compounds (Testosterone, Trenbolone, Dianabol) matched to user goals and safety profiles.
The Orals: Rapid Onset and Liver Strain
Oral anabolic steroids are structurally modified (C-17 alpha-alkylated) to survive passing through the liver without being destroyed. This allows for oral administration but introduces significant hepatotoxicity (liver stress).
1. Methandienone (Dianabol)
- Context: arguably the most famous oral steroid, popularized in the “Golden Era” of bodybuilding.
- Effect: It creates a rapid, dramatic increase in weight and strength, largely driven by glycogen loading and water retention. It is typically used as a “kickstarter” at the beginning of a cycle to see immediate results while waiting for slower-acting injectables to take effect.
2. Oxymetholone (Anadrol)
- Context: Originally developed to treat anemia.
- Effect: It drastically increases red blood cell count, improving muscular endurance and creating massive “pumps” during training. It is arguably the most potent oral for raw size, but also carries a high risk of blood pressure spikes and liver damage.
The Mechanism: Why Do They Work?
Regardless of the specific compound, anabolic steroids generally facilitate muscle gain through three primary mechanisms:
- Increased Protein Synthesis: They enhance the rate at which cells build proteins, allowing muscles to repair and grow faster than natural physiology permits.
- Nitrogen Retention: They prevent the catabolic (muscle-wasting) loss of nitrogen, keeping the body in an anabolic state even during calorie deficits or intense training.
- Red Blood Cell Production: By stimulating erythropoiesis, they increase the oxygen-carrying capacity of the blood, delaying fatigue and allowing for higher training volumes.
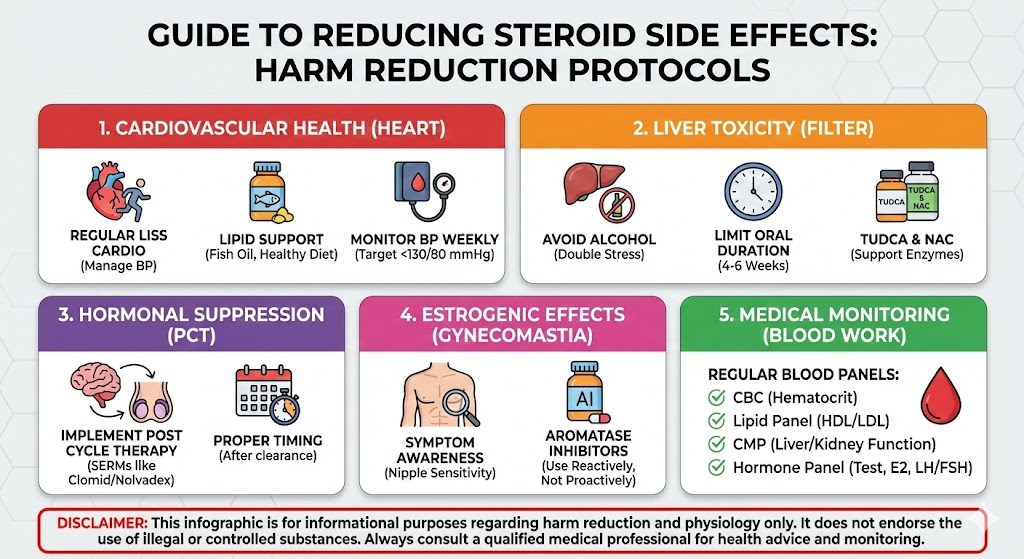
Health Risks
To discuss anabolics without discussing risk is to present an incomplete and dangerous picture. information must acknowledge the “biological debt” incurred by use.
- Hormonal Suppression: All anabolic use signals the body to stop producing its own testosterone. Without proper intervention (Post Cycle Therapy), this can lead to permanent hypogonadism.
- Cardiovascular Strain: AAS use is strongly linked to left ventricular hypertrophy (thickening of the heart walls), hypertension, and adverse lipid profiles (low HDL, high LDL).
- Psychological Effects: Fluctuations in hormones can lead to mood swings, aggression, or depression, particularly during withdrawal.
Conclusion
The landscape of anabolics is vast, ranging from mild compounds like Primobolan to harsh agents like Trenbolone. While they are undeniably effective at forcing the body to accrue muscle tissue beyond its genetic limit, they are not magic. They are powerful pharmaceuticals with systemic effects that extend far beyond the biceps and triceps.
For the vast majority of the population, the risks to long-term health—particularly cardiovascular and hormonal health—far outweigh the benefits of temporary muscle gain. True expertise in this field lies not just in knowing what these drugs do, but in understanding the severity of their consequences.



Leave a comment
Your email address will not be published. Required fields are marked *
You must be logged in to post a comment.